
|
Getting your Trinity Audio player ready... |
The third of our three ‘cancers of the month’ concerns the kidney. As the name implies, this type of cancer starts in the kidneys. Healthy cells in one or both kidneys grow out of control and form a lump, or tumour. It is one of the top 10 most common cancers in both men and women.
Signs and symptoms
Most people don’t show signs or symptoms in the early stages. Kidney cancer is usually found by chance during an abdominal imaging test for other issues. As the tumour grows, patients may experience:
- Blood in the urine
- Pain in the lower back
- A lump in the lower back or side of the waist
- Unexplained weight loss, night sweats, fever, or fatigue
Causes
We know that people are more likely to develop kidney cancer as they age. However, there are certain risk factors linked to the kidney cancer.
Some we can’t necessarily control, such as our gender -about twice as many men develop kidney cancer compared to women – or family history of the disease.
Other risk factors we can control, however :
- Smoking
- Being overweight (obese)
- High blood pressure
Kidney disease and kidney cancer
Studies show there is a link between kidney cancer and kidney disease.
Kidney cancer risk
Some studies show that people with kidney disease may have a higher risk for kidney cancer due to:
- Long-term dialysis: Some studies show that people on long-term dialysis have a 5-fold increased risk for kidney cancer.
- Immunosuppressant medicines: Some anti-rejection medicines that must be taken by kidney transplant recipients to prevent rejection can increase the risk of kidney cancer. It’s a Catch 22 situation, because without the immunosuppressant medicine the body will reject the new kidney.
Kidney disease risk
There is an identified link between kidney disease and kidney cancer. And it can be another Catch 22 situation.
- Radical nephrectomy (surgery): The entire kidney may need to be removed because the tumour is large and most of the kidney has been destroyed. The risk for kidney disease is higher if all (rather than part) of the kidney must be removed due to cancer. However, removing the whole kidney is often better for survival if the tumour is large or centrally located. For small tumours it is better to have surgery to remove the tumour but not the entire kidney (partial nephrectomy). This approach decreases the chance of developing chronic kidney disease and issues with heart and blood vessel disease.
- Drugs to slow or stop cancer growth: Drugs that spread throughout the body to treat cancer cells, wherever they may be, are sometimes used to treat advanced kidney cancer. All cancer drugs have some side effects, but some can be nephrotoxic, i.e. they can damage kidney function.
But remember, not everyone with kidney cancer will get kidney disease. Similarly, not everyone who has kidney disease or a transplant will get kidney cancer. The best approach is to lower the risks.
Types
Renal cell carcinoma (RCC) is the most common type of kidney cancer in adults. It usually starts in the lining of tiny tubes in the kidney called renal tubules. RCC often stays in the kidney, but it can spread to other parts of the body.
Clear cell renal cell carcinoma, also known as ccRCC or conventional renal cell carcinoma, is the most common form of kidney cancer, making up around 80% of all renal cell carcinoma cases. ccRCC is more common in adults than children.
Rare types of kidney cancer occur most frequently in children, teenagers, and young adults.
Papillary renal cell carcinoma (PRCC)
- 15% of all renal cell carcinomas
- Tumour(s) located in the kidney tubes
- Type 1 PRCC is more common and grows slowly
- Type 2 PRCC is more aggressive and grows more quickly
Translocation renal cell carcinoma (TRCC)
- Accounts for 1% to 5% of all renal cell carcinomas and 20% of childhood cases
- Tumour(s) located in the kidney
- In children, TRCC usually grows slowly often without any symptoms
- In adults, TRCC tends to be agressive and fast-growing
Benign (non-cancerous) kidney tumours
Benign, or non-cancerous kidney tumours grow in size but do not spread to other parts of the body and are not usually life-threatening. Surgical removal is the most common treatment.
- Papillary renal adenoma: The most common benign kidney tumour. Tumours are small, slow growing, often without any symptoms. Usually the are during an imaging test done for a different reason
- Oncocytoma: Tumours start in the cells of the kidney collecting ducts and can grow in one or both kidneys. They can grow from walnut to grapefruit size.
- Angiomyolipoma: Benign fatty tumours that can be be due to overgrowth of blood vessel and smooth muscle tissue cells. The tumours are non-cancerous, but can become very large and destroy surrounding tissue. Over a certain size they can cause internal bleeding
Prevention

General tips
- Don’t smoke
- Maintain a healthy weight
- Find out if you’re exposed to certain toxins at work or at home (such as cadmium, asbestos, and trichloroethylene, which may increase kidney cancer risk)
Be kind to your kidneys
As stated, people with kidney disease may be at increased risk for kidney cancer:
- 2 simple tests can help determine your kidney score:
- A blood test for kidney function (GFR)
- A urine test for kidney damage (ACR)
- Avoid prolonged use of non-steroidal anti-inflammatory drugs (NSAIDs) such as ibuprofen and naproxen
- Manage high blood pressure
- Manage blood sugar if you are diabetic
Be aware of other risk factors
- Family history of kidney cancer
- Certain diseases you may have been born with, such as von Hippel-Lindau disease
Diagnosis
Tests
Your doctor will diagnose kidney cancer by reviewing your medical history and doing a physical exam, along with blood and urine tests.
Imaging tests:
- Computed tomography (CT) scans use x-rays to make a complete picture of the kidneys and abdomen (belly). They can be done with or without a contrast dye. Small amounts of radiation are used. The CT scan often shows if a tumour appears cancerous or if it has spread beyond the kidney.
- Magnetic resonance imaging (MRI) scans make a complete picture of the kidneys and abdomen, but without radiation. They can be done with or without a contrast dye called gadolinium that should be avoided in people on dialysis or with very low kidney function.
- Ultrasound uses sound waves to give a complete picture of the kidneys and abdomen without radiation. It may be useful in helping to decide if a mass in the kidneys is a fluid-filled cyst or a solid tumour. This test is done without contrast dye.
A biopsy can be used in special cases, but is typically not recommended. A biopsy requires a very small piece of the kidney to be removed with a needle and then tested for cancer cells.
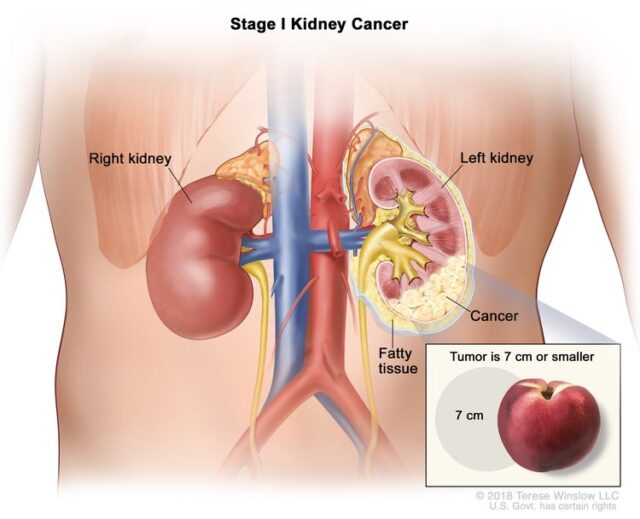
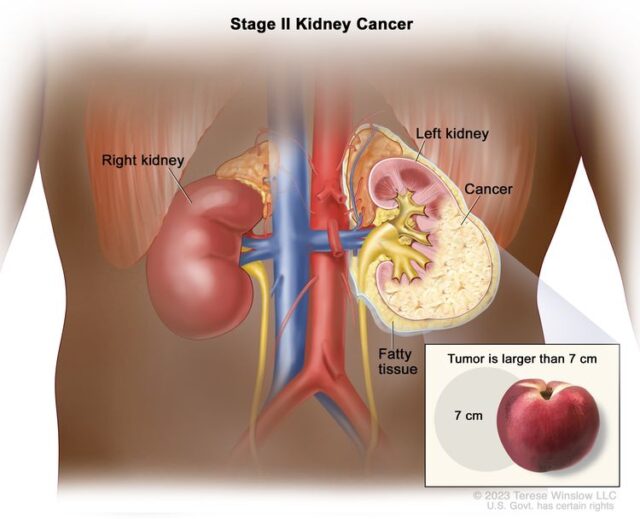
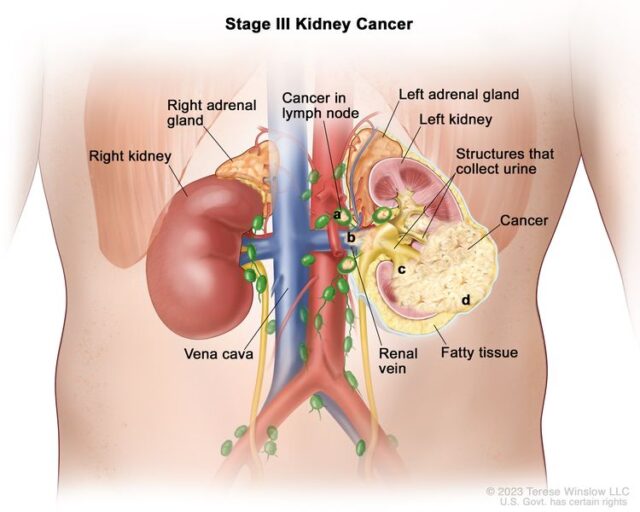
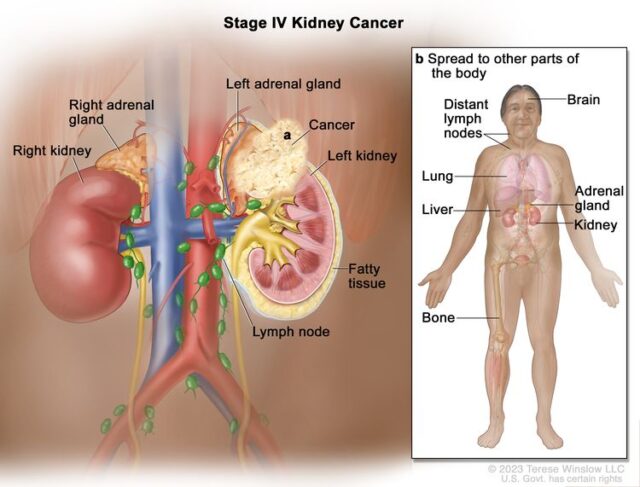
Stages
Once kidney cancer is found, tests will determin if the cancer has spread within the kidney or to other parts of the body, a process called staging. The higher the stage, the more serious the cancer.
Treatment
The most common treatment for kidney cancer is with surgery to remove all or part of the kidney. However, treatment will depend on the stage of the disease, as well as the patient’s general health, age, and other factors.
Surgery: Most people with early stage cancer (stages 1, 2, and 3) can be cured with partial or radical nephrectomy surgery. Surrounding tissues and lymph nodes may also be removed in the case of a radical nephrectomy.
Non-surgical options: Thermal ablation kills the tumour by burning or freezing and is most often used for small tumours in people who are not good candidates for nephrectomy surgery. Active surveillance is used if a small tumour is less than 4 centimetres (1.5 inches). Forms of chemotherapy and radiation used in other forms of cancer are not usually effective treatments for most forms of kidney cancer
Advanced or recurrent kidney cancer treatment: For people with advanced kidney cancer that has spread to other parts of the body, treatment with a drug may be recommended along with surgery, or instead of it. Advanced kidney cancer patients are living much longer than ten years ago.
- Medicine is often used for advanced kidney cancer that has spread to other parts of the body or where surgery cannot be carried out.
- Immunotherapy uses the body’s natural defences – immune system – to stop or slow the growth of cancer cells
- Monoclonal antibodies attack a specific part of cancer cells
- Checkpoint inhibitors help the immune system recognize and attack cancer cells
- Vaccines give an overall boost to the immune system
- Immunotherapy uses the body’s natural defences – immune system – to stop or slow the growth of cancer cells
- Anti-angiogenic therapies reduce the blood supply to a tumour to slow or stop its growth
- Targeted therapies directly inhibit the growth of the cancer
Nutrition
Good nutrition is essential during cancer treatment, getting enough calories and nutrients to help prevent weight loss and regain strength. Patients who eat well often feel better and have more energy.
Some people find it hard to eat well during treatment since it causes them to lose their appetite or have side effects like nausea, vomiting or mouth sores, which can make eating difficult. For some people, food tastes different.
Physical Activity
Kidney cancer patients should be encouraged to be physically active before, during, and after treatments, except for some temporary limitations after surgery. Physical activity during and after treatment has been shown to decrease anxiety, depression, and fatigue, while improving physical function, and health-related quality of life. Physical activity helps prevent frailty by keeping bones and muscles strong for good mobility, as well as proper heart and lung function. It also helps to control other health issues such as obesity, diabetes, and high blood pressure, all of which can affect the kidneys.
The American Cancer Society Guideline on Diet and Activity for Cancer Survivors 2022 recommends that physical activity assessment and counseling begin as soon as possible after diagnosis. The aim is to help patients prepare for treatments, tolerate and respond to treatments, and manage certain cancer-related symptoms and treatment-related side effects.1 The American Cancer Society and American College of Sports Medicine recommend that cancer survivors do 150 minutes of moderate aerobic physical activity per week or 75 minutes of vigorous aerobic physical activity per week, along with strength training at least two days per week on all muscle groups.
SO GUESS WHAT? GO CLIMBING!!
This is a summary of an article on the US National Kidney Foundation.
Main image courtesy nationalbreastcancer.org

